Friday, June 17th 2011
This is part of my Summer of the Pill series, where I will answer a question about the birth control pill every week for the summer. I will try and make them shorter than my usual posts. Please remember that I am not a medical doctor, so do not use this material to diagnose or treat any condition. I still hope you find these posts informative and useful.
One of the questions I got on my inaugural Summer of the Pill post is one that I have been asked many times over the years: Why do we menstruate, and is it even necessary while on the pill?
So first, let me back up and explain the modern birth control pill. Most of the standard, monthly pill packs have three weeks of synthetic hormones that you take daily. These hormones out-compete your natural ones, which is how they suppress ovulation. Over the course of these three weeks your endometrial lining is also building up some in response to these hormones. For many adult women in urban, or industrialized environments, the amount of synthetic hormone is lower than what their body would naturally produce, so the lining of the uterus is less thick than it would usually be.
The fourth week is a placebo week – you don’t have to take these pills, but you are usually encouraged to just so that you keep up the habit of taking a pill every day – and the absence of the synthetic hormones in your body triggers menstruation. Then you slough off the endometrial lining that was thickening and again, if you are one of the many adult industrialized women for whom the pill is designed, then you should actually have a lighter period than what you have in a natural cycle.
The placebo week in your standard pill pack is there because the original maker of the pill thought women would be disturbed by the absence of a period. And there are still many women who would prefer to get their period than not. But what about the women who would just as gladly stop menstruating at the end of each cycle or pill pack? Would this be a safe decision?
In order to get at these questions, I will answer three different ones for you: Why do we menstruate? What did we do back in the day? and What is appropriate today?
Why do we menstruate?
 |
| Adapted from Fleagle 1999 by me. |
Humans are not the only animals to undergo cycles of growth and regression in our endometrial lining. Yet, only a few animals actually menstruate. Menstruation has occasionally been observed in other great apes (this is the primate group where humans belong, with the chimps, bonobos, gorillas and orangs), and a few other animals. As far as we can tell, everyone else resorbs the lining before growing a new one. It seems to be that those animals who menstruate, do so because the amount of lining they have is greater than what they are able to resorb.
Then, even among those few other animals who have been occasionally observed to menstruate, only humans are copious menstruators. That is, we’re the only ones who seem to do it every time a cycle ends, in a large enough quantity that it is visible (and those of us in industrialized environments know it’s more than just visible – there is a whole section of the drugstore devoted entirely to pads, tampons and cups to help us dispose of it).
Most people seem to think that the reason humans have such thick endometria, that produce the byproduct of copious menstruation, is that we have big-brained babies with high oxygen and glucose needs. We have the most invasive trophoblast of all animals, where the selfish little bugger burrows its way right through the endometrium in order to set up shop and start making the placenta. And so the thickness and differentiation of the endometrium, as well as the precise timing of its readiness for implantation and network of blood vessels at the ready to feed that fetus, make it a highly specialized tissue of a rather significant quantity!
What did we do back in the day?
These days the average industrialized woman menstruates about 400 times in her life, and like I said, that menses is copious. Average menstrual blood loss is around 30mL, but anything below about 120mL is considered normal.
However, women in more traditional environments, particularly those who are foragers or pastoralists, menstruate far less frequently, only around 50 times (Strassmann 1997). Part of the reason for this is that their first period is much later in life, say around seventeen years old rather than twelve or thirteen, and that they expend a lot more energy and eat fewer calories each day (Strassmann 1997).
But there is another reason that the traditional environment, the one we assume humans evolved in, leads to far frequent menstruation: these women usually don’t have access to contraception, and thus practice what is called natural fertility. So the average number of live births for these women can be as many as eight, and even with high infant mortality that’s a lot of babies. Add to that the fact that these women will breastfeed through toddlerhood, and you have several menstruation-free years.
 |
| Figure 1. The industrial (top) versus nonindustrial (bottom) pattern of menstruation through the reproductive life span. The pink bars represent infrequent menses, the red bars represent frequent menses; breaks indicate no menses due to pregnancy and lactation. Note that the first period begins earlier in the industrialized pattern, and that fewer births, less breastfeeding, and more calories lead to more frequent menses across the reproductive years. |
So the industrial pattern doesn’t look anything like the nonindustrial, or traditional pattern. But the pill doesn’t necessarily look like either pattern – in terms of the number of menstruations it is like the industrial pattern, but in terms of ovulations it’s likely closer to the traditional pattern. The question is whether one of these patterns is necessarily healthier. I will partially answer this today.
What is appropriate today?
The placebo week of the pill is not necessary for contraceptive purposes, and the menstruation that occurs during this time may not be important for most women either. The two things worth talking to your doctor about are breakthrough bleeding, and the additional week of hormone exposure per month.
Breakthrough bleeding is when you have some kind of blood discharge at a time other than when you would expect to menstruate: when on the pill this would be any other time than the placebo week. And this can be very common in some populations even when using the normal pill preparations with the placebo week (Bentley 1996, Vitzthum et al 2001, Vitzthum and Ringheim 2005). Young users of the pill (say under 25 years old), athletes, and users from nonindustrial populations may be especially at risk.
If you have breast cancer or other reproductive cancers in your family history that are of the hormone-responsive variety, you may not want to expose yourself to any more hormone than you have to. The amount of hormone exposure in one’s life is correlated with risk of breast cancer (Jasienska and Thune 2001). However, the question of whether taking the pill helps or hurts your breast cancer risk is a very murky issue, and one that I will try to address in its own post later this summer.
Something you’ll read in this Summer of the Pill series is that making decisions about reproduction is about understanding trade-offs. You need to weigh the reasons you take the pill with the side-effects or negative impact of the pill, if you experience any. And many women out there could make up a pro/con list for taking the pill, or changing preparations, or skipping the placebo week, or changing to an IUD, and find that they weight each item very differently. There is rarely a single right answer.
References
Bentley, GR. (1996) “Evidence for interpopulation variation in normal ovarian function and consequences for hormonal contraception” in Variability in human fertility, eds L. a. M.-T. Rosetta, C.G.N. (Cambridge University Press, Cambridge, UK), pp 46-65.
Jasienska, G., & Thune, I. (2001). Research pointers: Lifestyle, hormones, and risk of breast cancer BMJ, 322 (7286), 586-587 DOI: 10.1136/bmj.322.7286.586
Strassmann, B. (1997). The Biology of Menstruation in Homo Sapiens: Total Lifetime Menses, Fecundity, and Nonsynchrony in a Natural-Fertility Population Current Anthropology, 38 (1) DOI: 10.1086/204592
Vitzthum VJ, Spielvogel H, Caceres E, & Miller A (2001). Vaginal bleeding patterns among rural highland Bolivian women: relationship to fecundity and fetal loss. Contraception, 64 (5), 319-25 PMID: 11777494
Vitzthum VJ, & Ringheim K (2005). Hormonal contraception and physiology: a research-based theory of discontinuation due to side effects. Studies in family planning, 36 (1), 13-32 PMID: 15828522
Tuesday, May 17th 2011
Sons and daughters and differential parental investment
One of my favorite rhetorical tricks is asking my students a question that has an obvious answer based on cultural expectations, but is wrong. So every year, when I start to teach my students about parental investment, I ask:
Who is harder to raise, sons or daughters?
I’ve asked by a show of hands and with iClickers, over the years, and the room of 750 is almost unanimous: daughters are harder to raise. So, then I get off the stage and walk around a bit. What do you mean by that? I ask.
Girls cause more gray hairs.
Girls cause more trouble when they start to like boys.
Girls are more work, and cost more money, since they shop all the time.
Girls talk back more.
And of course, there is always the saying that girls steal some of their mother’s beauty.
So then I show them this:
 |
| From Helle et al 2002. |
Here is a graph of maternal longevity based on the number of sons or daughters they have. This data was based on a historical population from Finland from 1640-1870 using church records (Helle et al 2002). As you can see, the more sons mothers bear, the shorter their lifespans. You see the opposite for daughters. So sons have a negative impact, and daughters have a positive impact. This same trend has been found in records from a Flemish village (van de Putte et al 2003, 2004), where sons negatively impact lifespan but not daughters. Interestingly, data from church records from the field site where I work in rural Poland provides a slightly different picture: every offspring of either sex reduced lifespan by about 95 weeks (Jasienska et al 2006).
 |
| From Jasienska et al 2006. |
Once students see these graphs, they quickly realize what is going on. Generally speaking, girls help mothers more at home in terms of chores and alloparenting. And in many cultures, particularly the historical ones studied so far, sons are costly because parents invest more in them, to help launch their own families. Daughters, not so much. In the Polish population, there may be other factors where daughter investment is important, or it is just costly to have so many offspring and you have maternal depletion regardless of daughter help.
Sex bias in parental investment is an important part of understanding both the biology and culture of parenting, and the developmental trajectories of children. The Trivers-Willard hypothesis, which has been tested many times in humans and animals, suggests that parents should invest more in sons when conditions are good, and more in daughters when conditions are bad. That is, when you have lots of resource you should put it towards a son in order to increase the chances he will have high reproductive success, since his is assumed to be more variable and high effort could lead to high reward. But in periods of low resource, daughters are a good bet because they are more likely to have at least some reproductive success no matter what.
 |
| From Hrdy 1990. |
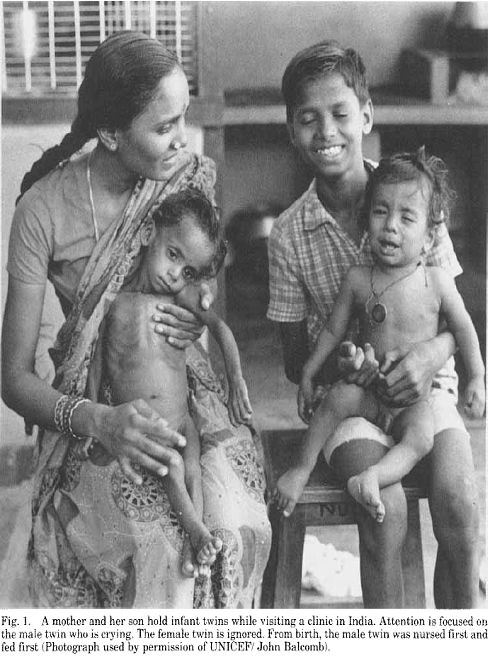
Of course, differential investment based on resources is further conflated in humans due to culture and, I would contend, our almost universal favor for patriarchy (Smuts 1995). Here is an image of an Indian family waiting at a clinic. There is a mother, an older son, and a twin boy and girl. Notice the extreme difference in health between the infant boy and girl – they are twins, yet the infant girl is emaciated. This is because in this population sons are always fed and cared for first, and whatever is left over, if there’s anything, is given to daughters.
So, parental investment can have real effects on the parent in terms of lifespan, and perhaps also their own future reproductive capabilities. Further, the conditions under which you may have children can vary, but how much a parent chooses to invest in their children varies too.
The piece of this that may be toughest to parse out, particularly in humans, is how the condition of the mother (or parents) can vary, and how that variation impacts the sex ratio of their children. In some species, like red deer, it is easier to imagine a mechanism: these animals have diapause, a period where their embryos are dormant until it is a good time to gestate and bear them. It is easier to insert some kind of selection process into a period where several embryos are all “frozen” and sex has been determined. But what about humans that produce singletons and invest huge, overlapping amounts of support to their children over decades? How would a sex bias based on maternal condition operate? And is there anything the offspring can do about it?
Changes in maternal breast size during pregnancy
It turns out that measurements as easy as stepping on a scale, and knowing your bra size, can begin to unpack the answer. First, a confession: I consider the author of this paper Andrzej Galbarczyk more than a colleague, but a friend. Andrzej is the graduate student who oversaw my Polish field site last season (Mogielica Human Ecology Study Site, director Dr. Grazyna Jasienska). He has translated consent forms and surveys for me and we’ve had many valuable and important conversations about my fieldwork. He is a smart, kind and thoughtful person and scholar. So, I let him see an early draft of this post to make sure I understood his point of view.
Galbarczyk performed an internet survey in Poland with 120 women, where he asked them to report their pre-pregnancy weight and bra size, their bra size directly after giving birth, and the sex of their offspring. He found two notable differences in these women: mothers of daughters weighed less before pregnancy, but had a greater changes in breast size during pregnancy.
The evidence about maternal pre-pregnancy weight is consistent with the Trivers-Willard hypothesis, as mothers who had sons were more likely to be heavier, and thus have more resource to invest. The second significant difference, that mothers with daughters had larger breasts after pregnancy, seems could be argued either way: Galbarczyk argues that it supports Trivers-Willard because mothers of sons could have been devoting more resource to growing their offspring rather than their breasts.
In other animals and primates particularly, mothers of male infants produce more energy-dense milk, yet mothers of female infants may produce a greater quantity of milk (Hinde 2009). And breast size is a pretty noisy signal of milk quality or quantity. So, what is the meaning of this difference in breast size?
Adaptation or physiological inevitability?
Galbarczyk suggests the difference is related to the evolutionary underpinnings of human female breasts. Women develop breasts around puberty, and though they certainly change in size and shape over time, keep them their whole lives. Other animals develop their mammary glands only shortly before lactating and then they regress again. Many contend that human breasts are an honest signal of fertility. This is at least partially confirmed by the correlation between breast size and estradiol concentrations (Jasienska et al 2006).
Galbarczyk thinks that the larger breasts seen in postpartum mothers to daughters may be a way to attract a mate for parental care. Perhaps this would help where she has given birth to the less-favored sex and needs to really convince him to participate; this could be a signal from the mother or the female fetus. Or maybe by appearing more attractive, she can have another reproductive opportunity, which would give her a chance to have a son.
You all know how I feel about evolutionary storytelling. In certain ways I do find this particular argument compelling, from the perspective of the Trivers-Willard hypothesis. But the evidence for the adaptive scenario around breast size is circumstantial.
Also, I don’t want this story to detract from some very interesting data: remember that Galbarczyk found that in this population, mothers of daughters weigh less before pregnancy, and develop larger breasts afterwards. Very cool. So perhaps we should consider a mechanistic, rather than adaptive explanation?
I have two thoughts about this, both related to androgens (androgens are the class of hormone that testosterone falls under). First, I wonder if there is an effect of fetal androgens from a male fetus on breast size. If so, mothers of daughters would have larger breasts simply because they aren’t having their breast tissue growth or density suppressed by androgens. It could simply be physiology that doesn’t have adaptive meaning.
Second, the mothers of sons were heavier before pregnancy. Heavier individuals tend to have higher circulating insulin levels, and the ovary can respond to higher insulin by producing more androgens (Poretsky 1991, Dimitrakakis et al 2004). So you could have a suppressive effect on breast size from that avenue as well. You don’t need an adaptive scenario for either of these mechanisms, just a consequence of how hormones work.
I would love to see Galbarczyk or someone else follow up on these thought-provoking results by measuring women, rather than relying on self-report, and by measuring their estradiol, progesterone and androgens. Understanding the different factors and motivations that lead to sex differential investment and outcome is a great field of study, and this work gets us thinking in a new direction.
References
Dimitrakakis C, Jones RA, Liu A, & Bondy CA (2004). Breast cancer incidence in postmenopausal women using testosterone in addition to usual hormone therapy. Menopause (New York, N.Y.), 11 (5), 531-5 PMID: 15356405
Galbarczyk A (2011). Unexpected changes in maternal breast size during pregnancy in relation to infant sex: An evolutionary interpretation. American journal of human biology : the official journal of the Human Biology Council PMID: 21544894
Helle, S. (2002). Sons Reduced Maternal Longevity in Preindustrial Humans Science, 296 (5570), 1085-1085 DOI: 10.1126/science.1070106
Hinde K (2009). Richer milk for sons but more milk for daughters: Sex-biased investment during lactation varies with maternal life history in rhesus macaques. American journal of human biology : the official journal of the Human Biology Council, 21 (4), 512-9 PMID: 19384860
Hrdy, S. (1990). Sex bias in nature and in history: A late 1980s reexamination of the “biological origins” argument American Journal of Physical Anthropology, 33 (S11), 25-37 DOI: 10.1002/ajpa.1330330504
Jasienska G, Nenko I, & Jasienski M (2006). Daughters increase longevity of fathers, but daughters and sons equally reduce longevity of mothers. American journal of human biology : the official journal of the Human Biology Council, 18 (3), 422-5 PMID: 16634019
Poretsky L, Seto-Young D, Shrestha A, Dhillon S, Mirjany M, Liu HC, Yih MC, & Rosenwaks Z (2001). Phosphatidyl-inositol-3 kinase-independent insulin action pathway(s) in the human ovary. The Journal of clinical endocrinology and metabolism, 86 (7), 3115-9 PMID: 11443175
Wednesday, April 20th 2011
When Dr. Grażyna Jasieńska invited me to give a talk on my thoughts around adolescents and hormonal contraceptives as part of an invited symposium on “Evolution through the Life Course,” I thought it was going to be an embarrassing experience, because I would not be presenting the quantitative data more common at the American Association of Physical Anthropology meetings. But I can’t say no to Grażyna, who has served as a wonderful mentor and cheerleader for almost ten years. Besides, if I can rant on a blog, surely I can let myself rant in a talk every now and then.
What follows is a bloggy version of the talk I gave Thursday the 14th, at the meetings in Minneapolis. Writing this post will, I hope, help me begin to turn this into a manuscript. Normally I wouldn’t dare write something on a blog that I would eventually want to publish. However, this is a piece that would benefit enormously from the kinds of conversations that happen in the science blogosphere. Further, I hope to publish it as an opinion piece well-studded with evidence. I think that by sharing my early thoughts now, my later thoughts will be more sophisticated.
* * *
Variation in adolescent menstrual cycles, doctor-patient relationships, and why we shouldn’t prescribe hormonal contraceptives to twelve year olds
 |
| From Vihko and Apter (1984). |
Vihko and Apter (1984) showed that there is variation in age at menarche, and that that variation tells us something about how long it should take an adolescent to start to achieve regular ovulatory cycles. The later your age at menarche, the longer you will experience irregular cycles. However, even in girls with ages at menarche twelve and under, it still took on average five years to achieve regular cycles. This indicates that, in adolescents, irregularity is in fact regular.
Lipson and Ellison (1992) have also looked at age-related variation in progesterone concentrations. Progesterone is the sex steroid hormone secreted by the ovary after ovulation, which is in the luteal phase. Luteal phase function is the one that seems to be the most variable within and between populations, and so progesterone is a great way to understand how female bodies vary. They found that those with the lowest hormone concentrations were on the extreme ends of their sample – 18-19 year olds, and 40-44 year olds and, as you might expect, hormone concentrations were higher as you moved towards the middle of that age range. So both younger and older women have low hormone concentrations relative to women in their reproductive prime, which is 25-35 years of age. But of course, this means that low hormone concentrations when you are in those early or late age ranges means that you are normal for your age.
 |
| From Lipson and Ellison (1992). |
Now, the United States has the highest rate of unintended teen pregnancy among industrialized nations. So I can understand why there are so many papers, and such a great effort, to get young girls on hormonal contraception (Clark et al. 2004; Clark 2001; Gerschultz et al. 2007; Gupta et al. 2008; Krishnamoorthy et al. 2008; Ott et al. 2002; Roye 1998; Roye and Seals 2001; Sayegh et al. 2006; Zibners et al. 1999).
But I’ve noticed two things: first, that hormonal contraception is used imperfectly in this population, with some estimates that 10-15% of adolescents on hormonal contraception still get pregnant (Gupta et al. 2008). Second, discontinuation rates for hormonal contraception in young girls are high, with many girls complaining about side effects, particularly breakthrough bleeding (Clark et al. 2004; Gupta et al. 2008; Zibners et al. 1999). I have to admit some concern over the fact that many of the papers I read that mentioned these discontinuation rates and side effects were almost condescending in their tone. The implication was that the side effects weren’t a big deal.
One of the ways clinicians and sexual health educators are trying to improve hormonal contraceptive use in adolescents is to emphasize their off-label use as a “regulator” – that is, the pill can regulate your cycle, regulate your mood, regulate your skin. The idea is to emphasize the positive effects of hormonal contraception to combat the side effects young girls both worry about, and actually experience. This also tends to produce campaigns and commercials with images of idealized young women that young girls would want to model themselves after – skinny, confident, and of course very feminine.
Despite the criticisms I’ve begun to name, there are substantial benefits to hormonal contraception in adult women. When women take hormonal contraception in adulthood, particularly in the 25-35 year range, they are very effective contraception. The pill also may reduce risk of reproductive cancers, though results are mixed (Collaborative Group 1996; Collaborative Group 2008; Kahlenborn et al. 2006; Marchbanks et al. 2002; Modan et al. 2001; Narod et al. 1998; Smith et al. 2003). And of course, off-label use to treat painful periods or premenstrual syndrome can be beneficial for many (Fraser and Kovacs 2003).
However, the benefits of hormonal contraception in adults seems to be limited to more industrialized populations. Bentley (1994; 1996) first raised these concerns. She discussed the possible genetic, ethnic and developmental differences between women that could produce variation in pharmacokinetics, which could in turn vastly change the experience and efficacy of hormonal contraception in a global context. Virginia Vitzthum and others have also shown that there are high discontinuation rates and complaints of breakthrough bleeding in rural Bolivian women on hormonal contraception (Vitzthum and Ringheim 2005; Vitzthum et al. 2001). Other studies have shown similar discontinuation rates and side effects in other non-industrial populations (de Oliveira D’Antona et al. 2009; Gubhaju 2009).
You might notice that the issues in non-industrial populations mirror what has been seen in industrial adolescent girls. This isn’t surprising, given that they also have in common fewer ovulatory cycles and lower hormone concentrations.
So, I worry about whether the clear benefits of hormonal contraception in adulthood can be applied to adolescent girls, some as young as eleven or twelve years old. With the imperfect administration and high discontinuation rates, they aren’t that great as contraception. But there are additional, physiological concerns. What are the effects of giving doses of hormones to young girls with newly developing hypothalamic-pituitary-ovarian axes? The variation I mentioned before, where irregularity is regular in adolescence, is because the feedback loop between the brain and the gonads is priming and developing in this period, and this takes time. The sensitivity of the feedback loop is being set. If we flood this feedback loop with extra hormone, does this alter its sensitivity? It is a question worth testing.
Further, if we flood this immature system that normally has irregular cycles and low hormones, are we increasing lifetime estrogen exposure? High lifetime estrogen exposure is a risk factor for breast cancer and other reproductive cancers. Is it possible that hormonal contraception in adolescence could have the opposite effect of hormonal contraception in adulthood? Again, we need to test this hypothesis.
Future work on this topic includes asking whether adolescent menstrual cycle variation is any different today than twenty to thirty years ago. The only data we have (at least that I know of) are from the aforementioned 1984 and 1992 papers, and maybe some derivative papers using the same datasets. But we all know there have been massive changes in body composition, diet and health in the last few decades that deserve consideration. So, this work needs to be re-done on a current population.
We also need to ask how adolescent reproductive functioning varies within and between populations. While this has been studied extensively in adult women, we don’t have a sense of adolescent population variation. This will give us a sense of what ecological variables produce variation not only in age at menarche, but in how long cycle irregularity persists and reproductive hormone concentrations.
Some additional, provocative, post-meeting thoughts
 |
| Bristol Palin. Image from here. |
In this symposium, Karen Kramer delivered a beautiful paper just before mine on teen pregnancy, and I had some great conversation with session participants and attendees, that has further evolved my own thinking on this issue. I want to say something just a little provocative:
While I think teen pregnancy should be avoided, culturally we overstate its dangers and consequences because we have a real problem with young people reproducing. This can lead young girls to overlook potentially more serious issues like sexually transmitted infections, HIV, and cervical cancer, all of which girls and women are at risk for if they use only hormonal contraception and have otherwise unprotected sex.
Let me explain two important points here. First, in most industrialized nations we are not set up well to support young mothers because of the way families are isolated, yet social support is a strong predictor of birth weight, postpartum depression, and labor progression (Collins et al. 1993; Feldman et al. 2000; Turner et al. 1990). So there are very strong and obvious reasons why teen pregnancy and motherhood can be incredibly challenging in industrialized environments. I wonder sometimes if that lack of cultural support is related to a fear that more young girls will get pregnant if they feel they have permission to procreate. This is similar to the argument in favor of abstinence-only sex ed: if they don’t know their options, or are shamed into believing this option is the worst possible one, then of course they won’t make them. But adults aren’t rational. I’m unsure why we expect adolescents to be.
We also need to consider population variation in adolescence and pregnancy. Variation in age at first birth in traditional populations is quite wide, from sixteen to almost twenty six years of age (Walker et al. 2006). In more traditional populations you see a lot of allomothering and grandmothering to support first time mothers, who are often teenagers (Hawkes 2003; Hrdy 2009; Kramer 2005; Kramer 2008). So, support systems are built in, and it does not alter the trajectory of your life in the same way teen pregnancy does in an industrialized population.
This range of variation in age at first birth, and the fact that most of those young mothers do just fine, perhaps even end up with higher reproductive success, leads me to my second point: the physiological evidence against teen pregnancy might be overstated. In her talk, Karen discussed a paper of hers in the American Journal of Physical Anthropology that described the negative health outcomes of teen pregnancy (Kramer 2008). In it, she reviewed literature that suggests that when you control for lack of prenatal care, first pregnancy, and low socioeconomic status, the common assumption that pregnancy is harmful to teens is significantly weakened.
Further, in her own work with Pumé foragers in Venezuela, mothers under the age of fourteen were the only group to have greater infant mortality than the referent group of late reproducers (Kramer 2008). Yet when we teach young girls about their bodies, we tell them that their bodies are not equipped to have babies in their teens and that there are extreme consequences (in fact, I have said exactly this in the past). The reality is that those consequences are worst for very young teens, and may not be as significant in older teens.
Am I advocating teenagers get pregnant? Absolutely and unequivocally no. But I think they need access to correct information, not skewed information. This means telling them the truth about our uncertainties about the health implications for hormonal contraception in adolescence, it means educating them about the importance of barrier methods, and it means making sure they understand the health risks associated with unprotected sex.
This is a nuanced issue that requires nuanced thinking. Despite my concerns about adolescent hormone contraceptive use, there are problems with barrier methods as well, particularly when there may be a cultural bias against their use, or in situations when women cannot safely use contraception in an obvious way with their partner (Gupta et al. 2008). Again, what is important here is conveying correct information, so that each individual can weigh the pros and cons as they relate to her own context. This means it could be an excellent idea for some twelve year olds to be on hormonal contraception, and a terrible one for other girls through the age of twenty. It is going to have to be up to them.
I hope this post generates some thinking and some conversation, and I welcome people who might push me in a different direction than where I’m currently thinking. I am sharing this now, before putting it together as a manuscript, to provoke thoughts and comments.
References
Bentley GR (1994). Ranging hormones: do hormonal contraceptives ignore human biological variation and evolution? Annals of the New York Academy of Sciences, 709, 201-3 PMID: 8154705
Bentley GR. 1996. Evidence for interpopulation variation in normal ovarian function and consequences for hormonal contraception. In: Rosetta LaM-T, C.G.N., editor. Variability in human fertility. Cambridge, UK: Cambridge University Press. p 46-65.
Clark, L. (2004). Menstrual irregularity from hormonal contraception triggers significant reproductive health fears in adolescent girls Journal of Adolescent Health, 34 (2), 123-124 DOI: 10.1016/j.jadohealth.2003.11.091
Clark, L. (2001). Will the Pill Make Me Sterile? Addressing Reproductive Health Concerns and Strategies to Improve Adherence to Hormonal Contraceptive Regimens in Adolescent Girls Journal of Pediatric and Adolescent Gynecology, 14 (4), 153-162 DOI: 10.1016/S1083-3188(01)00123-1
Collaborative group (1996). Breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies The Lancet, 347 (9017), 1713-1727 DOI: 10.1016/S0140-6736(96)90806-5
Collaborative Group on Epidemiological Studies of Ovarian Cancer, Beral V, Doll R, Hermon C, Peto R, & Reeves G (2008). Ovarian cancer and oral contraceptives: collaborative reanalysis of data from 45 epidemiological studies including 23,257 women with ovarian cancer and 87,303 controls. Lancet, 371 (9609), 303-14 PMID: 18294997
Collins, N., Dunkel-Schetter, C., Lobel, M., & Scrimshaw, S. (1993). Social support in pregnancy: Psychosocial correlates of birth outcomes and postpartum depression. Journal of Personality and Social Psychology, 65 (6), 1243-1258 DOI: 10.1037//0022-3514.65.6.1243
D’Antona Ade O, Chelekis JA, D’Antona MF, & Siqueira AD (2009). Contraceptive discontinuation and non-use in Santarém, Brazilian Amazon. Cadernos de saude publica / Ministerio da Saude, Fundacao Oswaldo Cruz, Escola Nacional de Saude Publica, 25 (9), 2021-32 PMID: 19750389
Feldman PJ, Dunkel-Schetter C, Sandman CA, & Wadhwa PD (2000). Maternal social support predicts birth weight and fetal growth in human pregnancy. Psychosomatic medicine, 62 (5), 715-25 PMID: 11020102
Fraser IS, & Kovacs GT (2003). The efficacy of non-contraceptive uses for hormonal contraceptives. The Medical journal of Australia, 178 (12), 621-3 PMID: 12797849
Gerschultz KL, Sucato GS, Hennon TR, Murray PJ, & Gold MA (2007). Extended cycling of combined hormonal contraceptives in adolescents: physician views and prescribing practices. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 40 (2), 151-7 PMID: 17259055
Gubhaju, B. (2009). Barriers to Sustained Use of Contraception in Nepal: Quality of Care, Socioeconomic Status, and Method-Related Factors Biodemography and Social Biology, 55 (1), 52-70 DOI: 10.1080/19485560903054671
Gupta, N., Corrado, S., & Goldstein, M. (2008). Hormonal Contraception for the Adolescent Pediatrics in Review, 29 (11), 386-397 DOI: 10.1542/pir.29-11-386
Hawkes, K. (2003). Grandmothers and the evolution of human longevity American Journal of Human Biology, 15 (3), 380-400 DOI: 10.1002/ajhb.10156
Hrdy SB. 2009. Mothers and others: the evolutionary origins of mutual understanding: Belknap Press.
Kahlenborn, C., Modugno, F., Potter, D., & Severs, W. (2006). Oral Contraceptive Use as a Risk Factor for Premenopausal Breast Cancer: A Meta-analysis Mayo Clinic Proceedings, 81 (10), 1290-1302 DOI: 10.4065/81.10.1290
Kramer, K. (2005). Children’s Help and the Pace of Reproduction: Cooperative Breeding in Humans Evolutionary Anthropology: Issues, News, and Reviews, 14 (6), 224-237 DOI: 10.1002/evan.20082
Kramer KL (2008). Early sexual maturity among Pumé foragers of Venezuela: fitness implications of teen motherhood. American journal of physical anthropology, 136 (3), 338-50 PMID: 18386795
KRISHNAMOORTHY, N., SIMPSON, C., TOWNEND, J., HELMS, P., & MCLAY, J. (2008). Adolescent Females and Hormonal Contraception: A Retrospective Study in Primary Care Journal of Adolescent Health, 42 (1), 97-101 DOI: 10.1016/j.jadohealth.2007.06.016
Lipson, S., & Ellison, P. (2008). Normative study of age variation in salivary progesterone profiles Journal of Biosocial Science, 24 (02) DOI: 10.1017/S0021932000019751
Marchbanks, P., McDonald, J., Wilson, H., Folger, S., Mandel, M., Daling, J., Bernstein, L., Malone, K., Ursin, G., Strom, B., Norman, S., Wingo, P., Burkman, R., Berlin, J., Simon, M., Spirtas, R., & Weiss, L. (2002). Oral Contraceptives and the Risk of Breast Cancer New England Journal of Medicine, 346 (26), 2025-2032 DOI: 10.1056/NEJMoa013202
Modan B, Hartge P, Hirsh-Yechezkel G, Chetrit A, Lubin F, Beller U, Ben-Baruch G, Fishman A, Menczer J, Struewing JP, Tucker MA, Wacholder S, & National Israel Ovarian Cancer Study Group (2001). Parity, oral contraceptives, and the risk of ovarian cancer among carriers and noncarriers of a BRCA1 or BRCA2 mutation. The New England journal of medicine, 345 (4), 235-40 PMID: 11474660
Narod, S., Risch, H., Moslehi, R., Dørum, A., Neuhausen, S., Olsson, H., Provencher, D., Radice, P., Evans, G., Bishop, S., Brunet, J., Ponder, B., & Klijn, J. (1998). Oral Contraceptives and the Risk of Hereditary Ovarian Cancer New England Journal of Medicine, 339 (7), 424-428 DOI: 10.1056/NEJM199808133390702
Ott, M., Adler, N., Millstein, S., Tschann, J., & Ellen, J. (2002). The Trade-Off between Hormonal Contraceptives and Condoms among Adolescents Perspectives on Sexual and Reproductive Health, 34 (1) DOI: 10.2307/3030227
ROYE, C. (1998). Condom use by hispanic and african-american adolescent girls who use hormonal contraception Journal of Adolescent Health, 23 (4), 205-211 DOI: 10.1016/S1054-139X(97)00264-4
Roye CF, & Seals B (2001). A qualitative assessment of condom use decisions by female adolescents who use hormonal contraception. The Journal of the Association of Nurses in AIDS Care : JANAC, 12 (6), 78-87 PMID: 11723916
SAYEGH, M., FORTENBERRY, J., SHEW, M., & ORR, D. (2005). The developmental association of relationship quality, hormonal contraceptive choice and condom non-use among adolescent women Journal of Adolescent Health, 36 (2), 97-97 DOI: 10.1016/j.jadohealth.2004.11.009
SMITH, J., GREEN, J., DEGONZALEZ, A., APPLEBY, P., PETO, J., PLUMMER, M., FRANCESCHI, S., & BERAL, V. (2003). Cervical cancer and use of hormonal contraceptives: a systematic review The Lancet, 361 (9364), 1159-1167 DOI: 10.1016/S0140-6736(03)12949-2
Turner, R., Grindstaff, C., & Phillips, N. (1990). Social Support and Outcome in Teenage Pregnancy Journal of Health and Social Behavior, 31 (1) DOI: 10.2307/2137044
Vihko R, & Apter D (1984). Endocrine characteristics of adolescent menstrual cycles: impact of early menarche. Journal of steroid biochemistry, 20 (1), 231-6 PMID: 6231419
Vitzthum, V., & Ringheim, K. (2005). Hormonal Contraception and Physiology: A Research-based Theory of Discontinuation Due to Side Effects Studies in Family Planning, 36 (1), 13-32 DOI: 10.1111/j.1728-4465.2005.00038.x
Vitzthum, V. (2001). Vaginal bleeding patterns among rural highland Bolivian women: relationship to fecundity and fetal loss Contraception, 64 (5), 319-325 DOI: 10.1016/S0010-7824(01)00260-8
Walker, R., Gurven, M., Hill, K., Migliano, A., Chagnon, N., De Souza, R., Djurovic, G., Hames, R., Hurtado, A., Kaplan, H., Kramer, K., Oliver, W., Valeggia, C., & Yamauchi, T. (2006). Growth rates and life histories in twenty-two small-scale societies American Journal of Human Biology, 18 (3), 295-311 DOI: 10.1002/ajhb.20510
ZIBNERS, A., CROMER, B., & HAYES, J. (1999). Comparison of continuation rates for hormonal contraception among adolescents Journal of Pediatric and Adolescent Gynecology, 12 (2), 90-94 DOI: 10.1016/S1083-3188(00)86633-4